


Zero Covid vs focussed protection: fantasy or reality?
Part 2 of the pandemic review asks whether the UK should have pursued one of the two most extreme Covid-19 policies


Other than perhaps the use of face masks, nothing has drawn so much ire or abuse as advocating for either a policy of trying to eliminate Covid-19 (so called, “Zero Covid”1), or removing all restrictions on younger people and focussing energy on trying to shield the elderly or vulnerable from infection (so called, “focussed protection”). These 2 extremes of Covid-19 policy were promoted in high profile articles which became nearly synonymous with their respective policy. The debate between the camps has rancorous and often personal.
Putting this aside, many people continue to argue the UK was at fault for not taking one or the the other path. We will examine both to determine whether there is any truth to these claims.
Should the UK have pursued “Zero Covid?”
New Zealand has so far had a highly successful pandemic response and is probably the poster child of Zero Covid for western democracies. It has managed to defer the majority of infections until its elderly population were comprehensively vaccinated. This has probably saved tens of thousands of lives.
The UK was never in a position to replicate the successful strategy of New Zealand.
Due to it’s deep international integration, the UK had significantly higher numbers of cases introduced earlier on than New Zealand. In addition, it was much easier for NZ to close their borders entirely due to their geographical isolation and nature of their trade (a substantial amount of goods arrive in the UK by road/ferry). This allowed NZ to close off at low levels of disease, snuff out the few infections they had, then seal themselves off from further introductions.
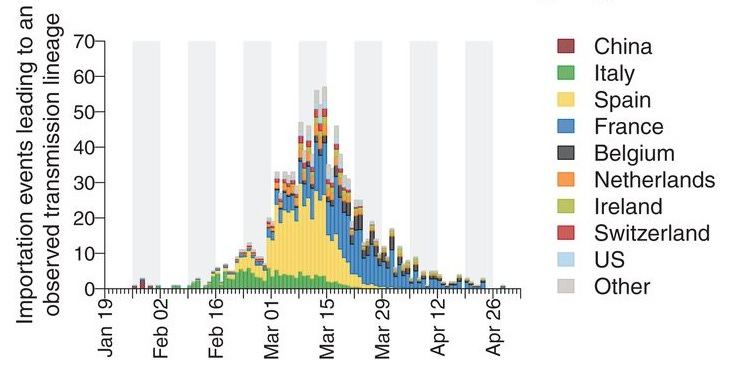
The chart above shows the number of cases introduced into the UK from various different locations during early 2020, as deduced by genetic sequencing.
The nature of the UK’s dependence on internationally integrated systems and trade (especially with Europe) makes complete border closure impossible (remember what happened over just 2 days of border closure with France at the end of 2020?). This, combined with the high levels of initial disease introduced into the country, made subsequently eliminating infection unachievable.
No countries achieved elimination following the high levels of disease initially experienced by the UK. It would have been desirable, but claims we could have eliminated Covid-19 had we just tried a bit harder, are not based in reality.
Australia managed to hold on for some time after a similar start to New Zealand, but ultimately even after the worlds longest lockdown, the state of Victoria had to give up and begin to reopen after it became clear that getting back to zero was impossible.
Other considerations
Further things to consider include, what if effective vaccines had not been established? This was far from guaranteed. One only needs to look to the tragedy which unfolded in Hong Kong to see what awaits countries who achieved Zero Covid, but did not manage to protect their elderly by the time Covid-19 finally got loose.
What are the ethics of testing vaccine efficacy in low income countries after wealthier ones manage to eliminate them?
All of this is before we even begin to examine the political landscape in which these decisions might have occurred, and the civil unrest which might have resulted from the truly extraordinary restrictions which would have been necessary to make a serious attempt at trying to achieve elimination within the borders of the UK. I will leave that for the political scientists and sociologists.
The Zero Covid strategy of New Zealand certainly had its own costs, in particular in regards to extremely harsh border controls. However this was the price for keeping life relatively normal for most of the interim prior to the introduction of vaccines, and undoubtedly saving many thousands of lives.
Unfortunately for the UK, Zero Covid was just an appealing fantasy.
For a more technical explanation on why getting to zero cases is so hard once you exceed more than a handful, I recommend this blog article from Professor Thomas House.
What about South Korea?
Many people erroneously include countries like South Korea or Japan in the Zero Covid box. Neither of these countries had a policy of elimination, although for long periods they were able to achieve low levels of disease.
They are not a model we could have initially followed in the UK.
South Korea and many East Asian countries have massive, complex, existing infrastructure for comprehensive track and trace systems (with robust and often harsh quarantine/isolation procedures) which we did not have in the UK. They also involve an extraordinary intrusion into personal privacy which I do not believe most people would be willing to tolerate in western democracies. We could have subsequently introduced more robust systems into the UK, but we did not. These systems allowed countries to manage low to moderate amounts of transmission without many wider restrictions for most of the pandemic.
Should we have pursued “focussed protection”?
In some sense, we did. This is true of most countries who were unable to achieve elimination. Elderly and vulnerable populations were given special guidance and dispensation, including additional advice/restrictions on social isolation, and were prioritised for access to tests, vaccines and therapeutics. It is all a question of the degree of protection on one end, and freedom on the other.
The idea that some ill defined section of society could be completely walled off and left free from risk, whilst the remainder would be fine living life completely as normal is a fallacy.
Huge levels of transmission will always find their way to vulnerable populations, as they cannot be cut off from the world, leading to unacceptable mortality. This would also lead to very large absolute numbers of deaths and morbidity even in young people (pre-vaccine) given the millions of people who would have been infected.
Whilst it is true for young adults that at an individual level the risk per infection of Covid-19 is quite low, once you multiply this risk by the many millions of people who would become infected within just a few weeks in the absence of any mitigations, this would result in an overwhelming amount of suffering and pressure on the health care system.
Summary
The UK should have provided more resources to reduce transmission, provided better protection for the elderly and vulnerable, and relaxed some draconian restrictions on young people - taking key elements from both ideologies.
That said, neither strategy in their idealised form were an option for the UK. Both are unfeasible, and aiming for either would have resulted in untold harms, either through disease or through the methods used to try and eliminate it.
It is very easy to say the UK should have done either, but serious and realistic attempts to outline how they could practically and realistically have been achieved and maintained have never surfaced.
There is a reason for that.
This was part two of the UK pandemic review mini series. For the introduction and to read other parts of this series, you can click here.
Please note I consider there to be 2 distinct Zero Covid ideologies:
Eliminate Covid-19 until sufficient vaccination of the population, then transition slowly into some state of “living with Covid”
Eliminate Covid-19 and attempt to maintain an indefinite state of elimination (perhaps until Covid-19 is eradicated completely?)
The second of these ideologies is now moribund outside of China and lacks any reasonable endpoint, so we will ignore it for today and focus on the first.
There's another issue with the idea of whether or not a New Zealand "prevention till vaccination" strategy will work. It requires some other, western, modern nation to actually have infections in order to develop the vaccine. It's fallacious to think that even if everyone could have actually prevented infection with NPIs, that it would have been preferred, because it would have to happen in perpetuity due to absence of a vaccine. New Zealand's "success" came at the cost they imposed upon themselves for the NPIs, and the cost that other nations, including the UK, bore to take the infections along with the vaccine development.
In short, you cannot have one without the other, that would be a fantasy.
My thoughts are that nothing we did made any difference other than slowing down the inevitable virus to infect most people. I disagree that we couldn't have had better focused protection prior to vaccination. If we could find money for furlough then instead of businesses laying off so many, we could have found funding to manage care homes with staff that didn't work in more than one facility. These staff could have been paid more for their sacrifice keeping away from family for 2 weeks at time. We could have provided accommodation for healthcare workers. There could have been a system of quarantine and/or testing after being with their families in order to return to work. FFP3/N95 masks should have been worn more frequently in high risk areas. (I know these weren't necessarily available, but this is part of the lessons we should be learning, isn't it?) Prior to testing being available, sensible policies such as staying away from work if you displayed symptoms. (Most people who got covid had at least one symptom.)
It's true that we couldn't completely separate healthy young people getting infected to eventually passing it to the vulnerable, I agree. However, we didn't avoid that from our lockdowns regardless, so focused protection, in my opinion should have been at least trialled. We should never have closed schools, playgrounds, swimming pools or limited outdoor activities. I think restaurants should have remained open for those who wished to utilised them. Many wouldn't choose to go based on their own person risk. We should have been able to decide for ourselves who we met and where we met. Given the risks were clearly a sliding scale as age increases.
I agree with large gatherings/crowds needing to cease, and shops requiring a certain number in at a time, (pre-vaccine), but not much else.
The biggest lesson that I wonder will ever be rectified, is that our healthcare facilities run on poor staffing levels. We don't have the people or structural healthcare resources, and each winter our systems hit boiling point. Upping our capacity to deal with covid and all other health matters in general is paramount to lessons learned.