

Not now, Ebola
Another viral haemorrhagic fever outbreak. This one is more serious.


As if the ongoing hantavirus cluster on a cruise ship were not enough, the world now has another viral haemorrhagic fever to contend with. On May 15th 2026, Africa CDC confirmed an outbreak of Ebola virus disease in Ituri province, northeastern Democratic Republic of the Congo (DRC). Less than 48 hours later it was declared a public health emergency of international concern (PHEIC), the highest level of public health threat. At the time of writing, over 300 suspected cases and at least 88 deaths have been reported, with sequencing confirming the Bundibugyo strain.
This is the DRC’s 17th recorded Ebola outbreak since 1976. And it comes with a particular complication: there is no approved vaccine or treatment for this strain of the virus.
This outbreak already looks to be highly problematic.
What is Ebola?
Ebola virus disease causes viral haemorrhagic fever (VHF), one of the most severe clinical syndromes in infectious disease. The, “Haemorrhagic” is so-called as these illnesses cause damage to blood vessels and the clotting system, leading to bleeding, organ failure, and a very high risk of death. Unlike Hantavirus, it belongs to the family of High Consequence Infectious Diseases (HCID), deemed so for their high mortality, lack of treatments, difficulty to detect and potential for spreading in the community.
Ebola is both interesting and terrifying. It belongs to the family Filoviridae -- filoviruses, from the Latin for thread. Under an electron microscope it is one of the longest viruses known, forming distinctive elongated filaments sometimes shaped like a shepherd’s crook or the number 6. It looks nothing like how we imagine most viruses.
The virus was identified in 1976 following simultaneous outbreaks in Sudan and in what is now the DRC. The Congolese outbreak occurred in Yambuku, a remote village near the Ebola River. The name is, by the discoverers’ own account, wrong: they wanted to avoid stigmatising Yambuku and chose a nearby river as a more neutral reference, but subsequently found it was not actually the closest river to the outbreak site. The name stuck anyway.
Four species cause disease in humans: Zaire, Sudan, Bundibugyo, and Tai Forest, and they are all quite different. Zaire is the most feared, with an untreated case fatality rate (CFR) around 79%, it is responsible for the largest and deadliest outbreaks on record. Sudan carries a CFR of around 54%. Bundibugyo, identified for the first time in Uganda in 2007, has a CFR closer to 32% - the fact this makes it the “mild” Ebola is a depressing thought.
One additional species worth mentioning is Reston virus. It infected laboratory workers in Virginia in 1989 who developed antibodies but never got sick. The alarming thing about Reston is that spreads through the air between monkeys (airborne Ebola…). Thankfully it doesn’t cause disease in humans.
The natural reservoir is fruit bats, which appear to catch the virus without becoming ill. The 2014 West Africa outbreak was traced to a two-year-old boy in Guinea who had likely played near a hollow tree colonised by bats. The virus transmits between humans through direct contact with bodily fluids of infected individuals. Ebola is not airborne in the conventional sense.
The virus does other weird things, such as persist in immune-privileged sites like the eyes, testes, and central nervous system, long after a person has clinically recovered. Cases of sexual transmission from male survivors have occurred more than a year after recovery. A Scottish nurse even developed Ebola meningitis nine months after being discharged. This persistence in survivors is one reason response efforts cannot just stop when a patient leaves hospital.
In central Africa, funerals are a major driver of spread. Traditional washing and preparation of bodies, combined with extremely high viral loads in the deceased have made funeral practices a repeated amplifier in nearly every outbreak. Safe and dignified burial programmes are now a core pillar of the response.
Despite all this, most of the world paid little attention to it for the first three decades after its discovery. Ebola killed roughly 1,500 people in total across small, geographically isolated events, contained through case isolation and contact tracing. The disease was seen as too rare and too remote to justify pharmaceutical investment, and vaccine development stalled.
Then came 2014.
What 2014 changed
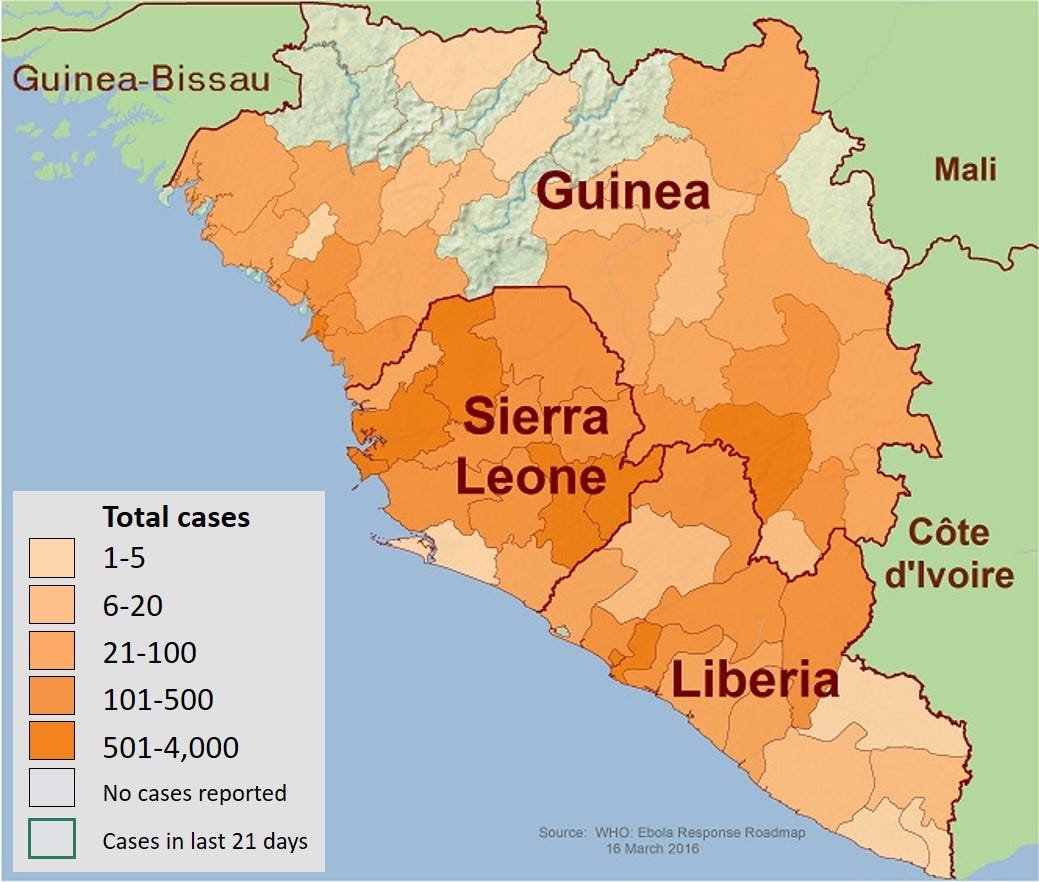
The West Africa outbreak of 2014 to 2016 infected more than 28,000 people across Guinea, Liberia, and Sierra Leone, and killed over 11,000. It grew in urban centres with weak health systems, overwhelmed the response capacity of three countries, and spread internationally, including infections of healthcare workers in Spain and the United States. By any measure, it was catastrophic.
It was also the event that finally triggered the development of effective countermeasures. Two vaccines are now licensed: rVSV-ZEBOV (Ervebo) and the two-dose Ad26.ZEBOV/MVA-BN-Filo regimen, and a monoclonal antibody combination (Inmazeb) has substantially reduced mortality (in clinical trials at least). Crucially, modern supportive care has significantly improved outcomes even without specific antivirals. Many historical “Ebola deaths” were really deaths from dehydration and electrolyte derangement that intensive care can correct. With supportive care and monoclonal antibodies, Zaire-strain mortality has been brought below 35% in trials.
All of which is good news. Except every approved countermeasure targets the Zaire strain.
The current outbreak
The outbreak is centred on Ituri province, in the remote northeast of the DRC. Ituri sits over 1,000km from Kinshasa, borders both Uganda and South Sudan, and is currently experiencing active conflict between rival militia groups. A healthcare worker was the first known case, with symptom onset on 24th April with fever, bleeding, vomiting, and severe weakness, and subsequently died at a medical centre in Bunia, Ituri’s capital. WHO was alerted to an unknown illness causing high mortality in Mongbwalu health zone on 5th May, including the deaths of four healthcare workers within four days of each other. The outbreak was officially declared on 15 May. On 17th May, WHO declared it a PHEIC.

An important detail from the early outbreak has emerged. Initial samples tested negative for Ebola. The available rapid tests detected only Zaire ebolavirus, not Bundibugyo, and a positive Bundibugyo result was not confirmed until 14th May - nearly six weeks after symptom onset in the index case, three weeks after the first cluster of healthcare worker deaths. There is speculation that the detection delay may be linked to recent cuts to global health programmes. That speculation will need to be assessed properly in due course, but the basic point is that the tools deployed to detect the outbreak could not detect the strain causing it.
It was caught late, and it was caught late for a specific reason.
The case counts reflect this delay. As of 18 May, DRC has reported 10 confirmed cases, 336 suspected cases, and 88 deaths, across at least nine health zones in Ituri. A separately confirmed case has been reported in Kinshasa (in someone returning from Ituri), and another in Goma, a city in North Kivu currently under the control of the March 23 Movement, which adds a substantial complication to contact tracing and response efforts.
Concerningly, Uganda has confirmed two cases in Kampala, with one death, in individuals who arrived from DRC within 24 hours of each other and have no apparent link, suggesting more than one importation chain. An American healthcare worker who had been caring for patients in the DRC tested positive on 17th May and is being moved to Germany for treatment. The US has implemented enhanced travel screening and entry restrictions for travellers from DRC, Uganda, and South Sudan.
The geography compounds everything. Mongbwalu is a high-traffic mining town, and the working hypothesis is that the outbreak originated there before patients moved to Rwampara and Bunia seeking medical care. Ituri has over 270,000 internally displaced people and 1.9 million people identified as being in humanitarian need. The combination of high population mobility, active conflict disrupting health infrastructure, an urban hotspot, an outbreak straddling territory controlled by different armed groups, and the geographical proximity to Uganda and South Sudan creates the conditions under which small outbreaks readily become large ones. WHO has been explicit that the true scale of the outbreak is likely larger than the reported figures, on the basis of the high positivity rate in initial sequencing (eight positives in 13 samples), the unusual clusters of community deaths being reported across multiple health zones, and the rising trend in syndromic surveillance.
The current situation is bad, and is likely to look worse as more information becomes available.
Worth noting in the middle of all this: Jean-Jacques Muyembe, the Congolese virologist who co-discovered Ebola in 1976 as a young doctor drawing blood samples in Yambuku, now heads the DRC’s National Institute for Biomedical Research and is on the response. The man who helped identify the virus is leading the response to it fifty years later, in the same country. It is one of the more remarkable careers in modern infectious disease.
Why this one is harder
The current outbreak is Bundibugyo, not Zaire. Global vaccine stockpiles exist for Ebola, but the vaccines in it were not designed to protect against this strain. There are no approved treatments. Africa CDC has convened an urgent coordination meeting with health authorities from DRC, Uganda, and South Sudan alongside pharmaceutical companies including Merck, Gilead, Regeneron, and Moderna, plus CEPI and Gavi, to assess what options exist. CEPI has indicated it can support accelerated trial facilitation if required. For now, the response depends on the classical pillars: case isolation, contact tracing, safe and dignified burials, and community engagement.
The lower CFR of Bundibugyo (32% vs Zaire’s 79%) is a silver lining (if you can call it that). If a third of confirmed cases die rather than four-fifths, the clinical picture looks different. This may add to the explanation of why the outbreak grew so large before being detected, if early cases were attributed to other causes. However, it certainly does not make this a minor outbreak.
The mode of transmission of Ebola means this is extremely unlikely to become a serious, sustained transmission risk in Western countries. Even during the 2014 outbreak, the UK only saw three cases which were all in healthcare workers looking after patients with Ebola. However, frontline staff around the world will once again be on high alert for gastrointestinal symptoms in travellers returning from central Africa.
Despite the fact this outbreak already significantly more deadly than the cruise-ship Hantavirus outbreak, it is likely receive receive a fraction of the media attention - unless cases end up on our doorstep.
Summary
Ebola is a filovirus which causes devastating viral haemorrhagic fever, and Bundibugyo is one of four species pathogenic to humans - less lethal than Zaire but still very serious. It was under-researched until the 2014 to 2016 West Africa outbreak finally drove the development of effective vaccines and treatments, but those tools are specific to Zaire. The current DRC outbreak involves Bundibugyo, was detected late, sits in a conflict-affected region with high cross-border mobility, and has already spread to Uganda. The response is now reliant on the same set of public health interventions that were available in 1976. Since Ebola spreads through close contact with bodily fluids and has never sustained transmission outside Africa, the risk to Europe or North America remains very low. The people at serious risk are those living in Ituri and the neighbouring provinces of Uganda and South Sudan, and, as always, the healthcare workers responding under extremely difficult conditions.