

Making Rash Decisions
When to worry about rashes when a child is sick


When your child is feeling unwell with fevers, one of the most striking features that may occur is the onset of a rash. This is a common cause of alarm among parents and a frequent reason for attending the emergency department. Fortunately, most of these rashes are completely benign and require no intervention; but how are parents supposed to know the difference?
Let’s walk through the issue together and bust some myths along the way!
The non-blanching rash
Let’s start with the rash which doctors will always want to review your child for. Almost all of the benign rashes share the same feature, which is that they blanch. This is indicative that the redness is caused by inflammation in the skin, and by an immune response to some other pathogen. The commonly known way of assessing this is the glass test - pressing a glass on the skin and seeing if the redness subsides. You can also stretch the skin for the same effect, and in practice I find this is actually much easier.
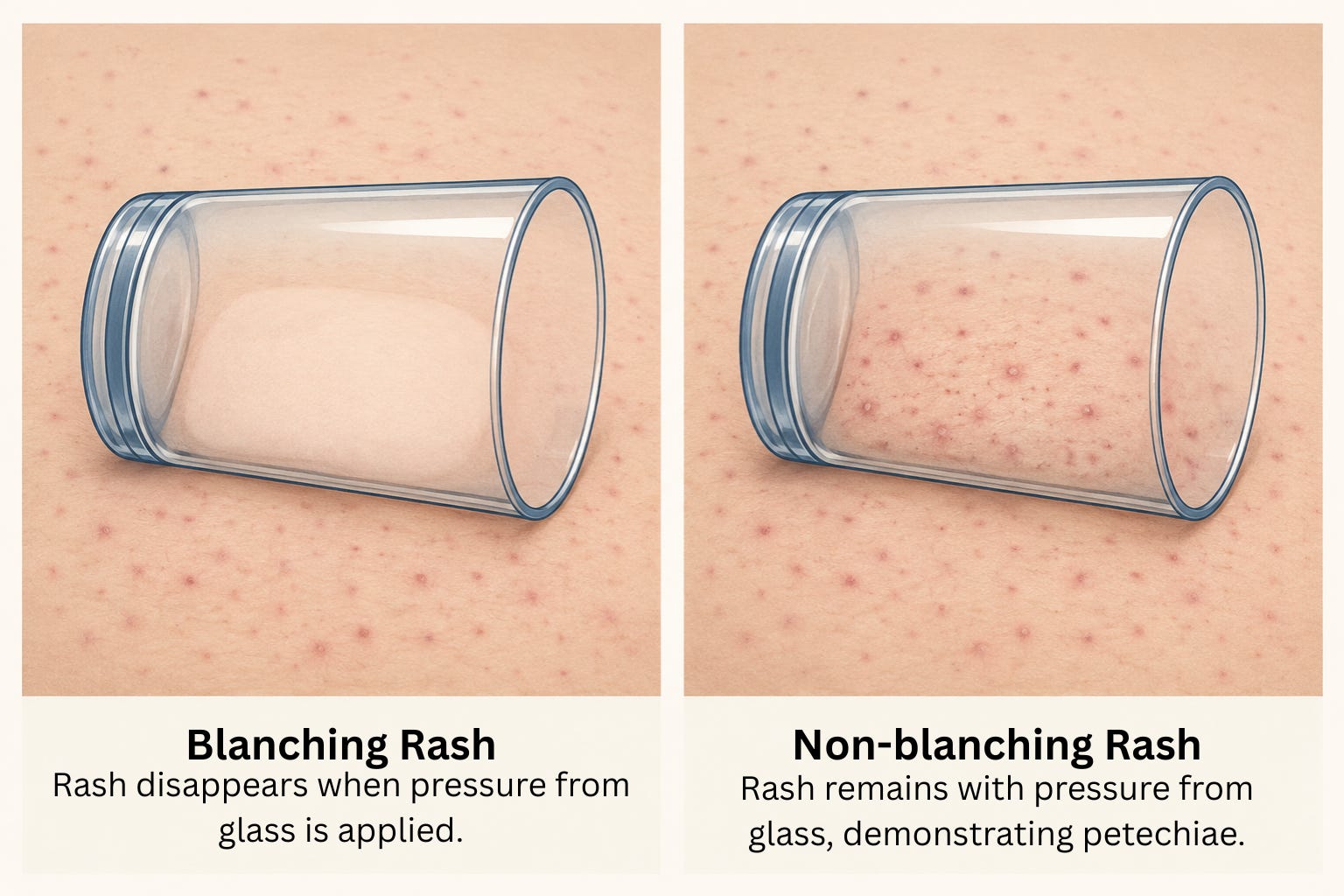
When a rash does not blanch, this is a sign of a different underlying cause. This indicates that blood has left the tiny blood vessels known as capillaries, and what you are seeing is actually tiny little bruises. When these spots are very small, we call them petechiae. When they get larger and start to coalesce, we call this purpura. At this point it looks like large bruises.

The most common cause of petechiae is just a viral infection, so it is probably nothing serious - however there is now enough of a chance that the rash is caused by something worth knowing about that a doctor would want to see them and probably do some basic blood tests.
The famous cause of this type of rash is Meningococcal septicaemia; a blood stream infection caused by Neisseria meningitidis, the bacteria famous for causing sepsis and meningitis. It was this bacteria that led to the highly successful awareness campaign around the glass test.
Thanks to the success of vaccination, it is now extremely rare for these rashes to be caused by Meningococcus. The latest studies suggest ~1% of all cases are attributable to this, with other invasive bacterial infections now being more common than Meningococcus, and benign viral infections being substantially more common than both. This is especially the case for petechiae; for purpura, the rates of Meningococcal disease and other invasive bacterial infections is much higher, and febrile children with purpura should be treated as though they have meningococcal disease until it can be proven otherwise.
It is worth doing blood tests for children with petechiae to investigate for Immune Thrombocytopaenic Purpura (ITP), which is a relatively benign condition when the immune system temporarily targets and consumes the small cells known as platelets which help your blood to clot. In very rare instances, non-blanching rashes with fever can also be the presenting symptom of leukaemia. Whilst being very rare, it is simple enough to rule this out with a quick blood test and is worth doing.
The Viral Exanthem
When kids are unwell with febrile illnesses, there are several different reasons a rash can occur but one of these is by far the most common. The type of rash we call, “viral exanthem”, occurs frequently during a multitude of different childhood viral illnesses being caused by several different pathogens. This category broadly covers the widespread, red, blotchy rash than can occur all over the body, and has the notable feature of being blanching (as discussed above).

The true biology behind why these rashes occur is not well known, but it appears to be a side effect of the immune response to the infection. The skin being the largest organ in the body means that it is often first to get caught in the cross-hairs when the immune system gets a little over-active.
The important thing about viral exanthems, is that despite having such a fancy name, they are almost completely benign, and absolutely no intervention is required.
There are multiple specific syndromes which can be diagnosed under this umbrella, but it is usually irrelevant (save a couple of cases mentioned below). Whether the child has Roseola, Slapped cheek syndrome, or some random enterovirus or adenovirus doesn’t change the fact that there is no effective treatment available, or needed, as these conditions are all benign and self limiting.
There are only two exceptions to this:
Measles: What used to be one of the most common and dangerous causes of viral exanthems in children is now relatively rare, but sadly, is becoming increasingly less rare in many western countries. If you suspect your child has measles, they absolutely must be seen by a health professional. It is a potentially dangerous infection, and it is important that public health authorities are able to trace and contain potential exposures. The most important risk factors for measles are vaccination history and known/possible exposure. The three C’s precede the rash (cough, coryza, conjunctivitis). It’s a shame this is even worth mentioning, but that is the world we are now living in.

Scarlet Fever: This falls into the category of viral exanthems for historical reasons, despite actually being caused by a bacteria - Group A Strep (GAS). This infection is not dangerous, but is caused by a strain of GAS which produces toxins and is associated with outbreaks of invasive disease. The hallmarks of scarlet fever are the sandpaper-like touch of the rash, which has a very rough texture to the skin, alongside a strawberry tongue. This is worth treating to prevent spread of the toxin producing strains of the bacteria, but the infection is not considered dangerous to the child themselves.
Urticaria
Most people are aware of the rash urticaria, commonly referred to as hives. It is known for being associated with allergy; but a fact that surprises most parents it the most common cause of this rash in children is viral infection! The rash can occur during or shortly after the infection itself, and is painless but can be itchy and troublesome. The main issue is that unlike allergic urticaria, viral urticaria is not effectively treated by antihistamines. In fact, it doesn’t seem effectively treated by anything at all. This can be irritating for the family, but is not a cause of any danger.
This rash can also last a surprisingly long time; often up to a week after onset. It is rarely a cause for concern and will resolve without any intervention.
One again, the cause is likely the skin receiving friendly-fire from the immune system responding to the initial infection.

Kawasaki disease
A last word on one non-infectious cause of fever and rash worth knowing about, as early in the illness it can look indistinguishable from viral exanthem. There is a rare condition caused by inflammation of blood vessels known as Kawasaki disease. Every child with fever for 5 days or more should be reviewed by a doctor to check for the symptoms of Kawasaki disease, which include; maculopapular rash (like a viral exanthem), large cervical lymph nodes, bilateral non-purulent conjunctivitis, strawberry tongue (or other oral mucosal changes), and peeling of the skin on the hands and feet. Children with Kawasaki disease are also usually absolutely miserable.
This condition is very rare, but can result in bulging of the coronary arteries with long-term complications if not diagnosed and treated early. It’s easy enough to remember that if your child has fever for 5 days or more, you should get them checked.
So when should I worry?
The rash is not the most important symptom. The key element is how your child seems in themselves. If they are behaving as you would expect with a usual childhood illness, then it is unlikely there is anything to worry about. If they have a blanching rash and they seem well, they probably don’t need to be seen unless you are worried they might have measles or scarlet fever.
Children with non-blanching rashes should always been seen by a doctor. It is most likely that this is still caused by a benign viral illness, but it is worth ruling out more serious causes.
Children with a fever for 5 days or more should be seen to check for the signs of Kawasaki disease, which although very rare, has complications which can be prevented if caught early.
The golden rule always applies. If your parental spidey-sense is tingling, it is always better to get them seen.
For more information on rashes, you can refer to the Healthier Together NHS page about rashes in children.
Fever and rashes were probably the most frequent reasons for parents bringing their children to the urgent care centre where I worked as a nurse practitioner. My approach was always the same, rule out meningitis, measles, rubella, chickenpox and scarlet fever. However, I did see a 10 year old with shingles and I’ve heard the youngest child diagnosed with shingles was 8 years old, I suspect that children are exposed to chickenpox in preschool, certainly I didn’t get chickenpox until I was 8 years old in the mid 1960’s.